By Ondine Quinn, MSW, CSW, CSE, Senior Director of Programs at Provide, Inc., with contributions from staff at the National Resource Center on Domestic Violence
Who are the most impacted by abortion bans and restrictions?
Abortion is essential health care. The Guttmacher Institute published an article in 2023 describing the inequities in US abortion rights and access based on racism and discrimination. In it they state:
“New and impending abortion restrictions and bans will undoubtedly deepen the profound inequities in abortion access that have long marked the reproductive health and well-being of pregnant people and their families. Not only Black, Latino and Indigenous people and people living with low incomes, but transmen and nonbinary people, immigrants, adolescents and people living with disabilities are all particularly likely to encounter compounding obstacles to abortion care and be harmed as a result.
Discrimination and denial of resources, rights and information on the basis of sexuality, race/ethnicity, gender, age, citizenship status and disability uniquely shape abortion access for people subject to intersecting forms of discrimination. For example, Latina, Black and Indigenous women are at the lowest end of the wage gap, earning about half the wages of White men, on average. They are therefore less likely than other groups to be able to overcome the egregious, unnecessary web of barriers to abortion care, both because they are less likely to have the money to do so and because they are more likely to experience racism in health care. Indeed, the effects of these interlocking systems of oppression—in which social and economic resources, safety and opportunity are distributed along lines of gender and race simultaneously—on access to contraception and abortion are compounding, not simply additive” (Fuentes, 2023).
How are people being criminalized for the abortions?
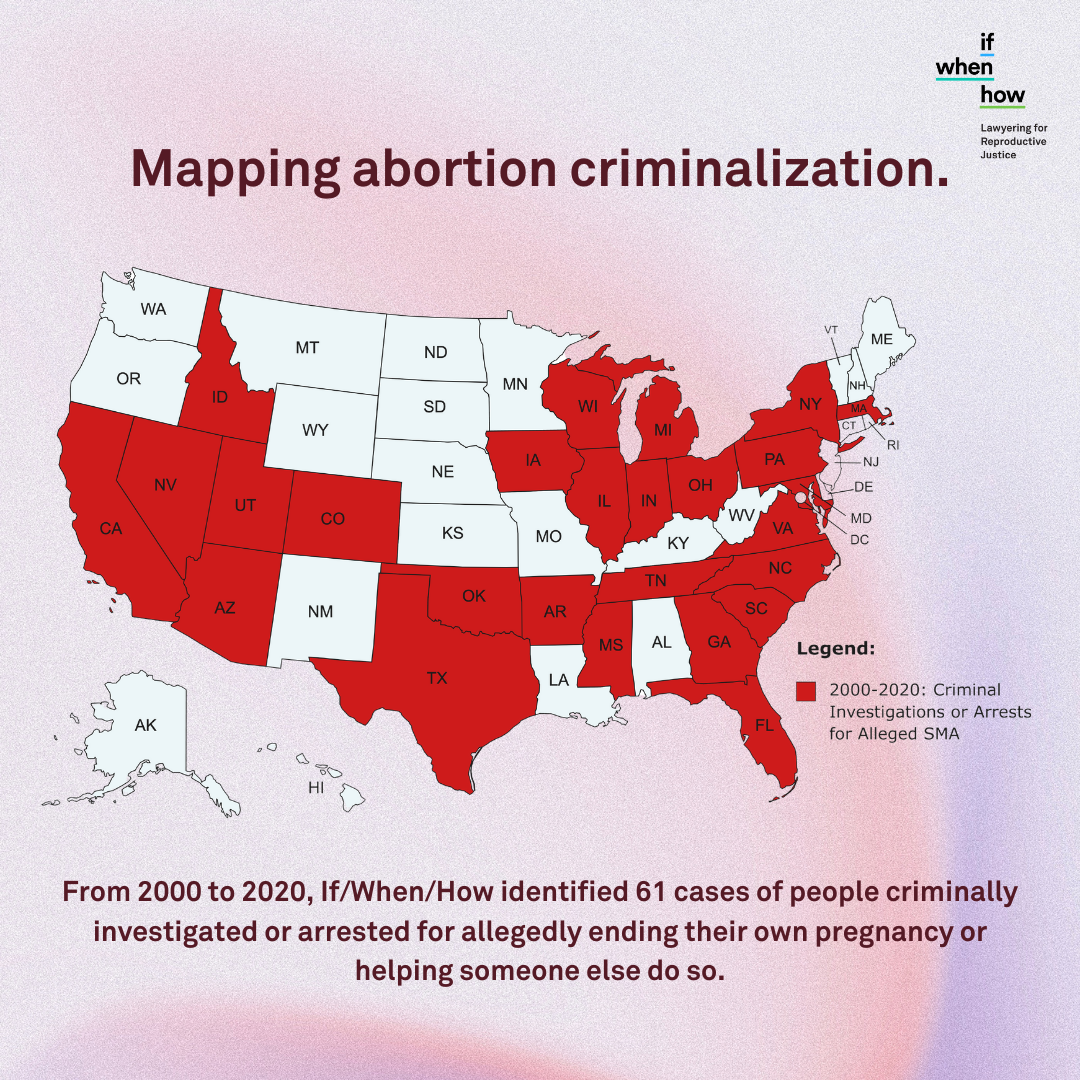
If/When/How recently published findings (2022) from a multiyear study around the criminalization of people ending their own pregnancy. One thing they found was that the primary privacy risk for people seeking abortion is other people. Forty-five percent of people were reported to police by health care providers or social workers. This is worth reading again—almost half of the reporting is being done by people who work in healthcare or social services, people who in many instances are guided by ethical and professional codes to do no harm and honor people’s autonomy. We don’t believe that most providers making these reports are doing so out of a desire to harm clients, but rather a lack of information about what, if any, mandatory reporting requirement exists.
Why does abortion access matter for survivors?
Conversations about pregnancy options, including abortion care, should be a regular part of working with survivors. People who can become pregnant may be at an increased risk of experiencing violence from an intimate partner during pregnancy. Further, many survivors have experiences with reproductive coercion. Reproductive and sexual coercion includes explicit attempts to impregnate a partner against their will, control outcomes of a pregnancy, coerce a partner to have unprotected sex, and interfere with contraceptive methods. These behaviors are intended to maintain power and control.
Approximately 20% of women seeking care in family planning clinics who had a history of abuse also experienced pregnancy coercion and 15% reported birth control sabotage (American College of Obstetricians and Gynecologists, 2012).
A 2019 study conducted by researchers at University of Pittsburgh and Michigan State University (MSU) found that nearly one in eight sexually active young women between the ages of 14 and 19 had experienced reproductive coercion. A survey of more than 3,000 people conducted by The National Domestic Violence Hotline found that 25% of participants had experienced this type of abuse in some form.
“He has tried to talk me into having a child. He told me he wanted to keep me from leaving him.” – Survivor surveyed by the Hotline
What is Self-Managed Abortion (SMA)?
With the changing legal landscape around abortion access, you may be hearing more in the news and from those you work with about “self-managed” abortion (SMA). For context, SMA broadly refers to non-clinical abortion, or abortion that happens outside of the formal healthcare system and without the involvement of a medical professional. SMA is not a back-alley abortion or a DIY abortion. It is an abortion that happens most commonly in someone’s home, done in privacy and safety, often with the help of a friend, family member or caregiver.
The Guttmacher Institute estimates that medication abortion accounts for more than half of abortions in the U.S. Misoprostol (alone or in combination with mifepristone) is a safe and effective way to end a pregnancy in the first 10 weeks and has been used successfully by people all over the world without a clinician.* SMA using abortion pills outside of a clinical setting is an option that enhances reproductive autonomy, while also potentially serving as a workaround to restrictive policies and gaps in access. While there is limited data on how common self-managed abortions are that don’t involve a medical provider at all in the U.S., there are reports that it does happen and abortion providers say that SMA may rise as access to care decreases.
*The safety of SMA with these medications does not mean that it is without risk or possible adverse reactions. For important considerations, see “Please Keep in Mind!” section.
Support, Don’t Report: Working with People Who Choose Self-Managed Abortion
Attend training on how to avoid criminalizing survivors.
![]()
To address this disturbing problem, Provide and If/When/How teamed up to offer training and technical assistance to domestic violence and sexual assault organizations on how to navigate mandatory reporting requirements to best support survivors who may consider self-managed abortion. We chose to focus our efforts on these organizations first because of the connections between partner violence, reproductive coercion, and the need for safe accessible abortion care—particularly for those most vulnerable to marginalization and oppression, like Black, Indigenous and other People of Color, LGBTQIA people, and low-income communities.
In these trainings, there is some values clarification work, we cover what self-managed abortion is and isn’t, the impact of criminalization of pregnant people and their families, the difference between giving legal advice and information, and most importantly, that there is no requirement presently in any state to report someone who is self-managing their abortion.
With the ever-changing legal landscape around abortion, and diminishing access to in-clinic abortion services, knowing how to support people who are considering self-managed abortion will become increasingly important. Provide intends to continue bringing this critical information to healthcare and social service providers across the country, particularly those who work in communities most impacted by legal barriers to care.
Share resources with fellow advocates.
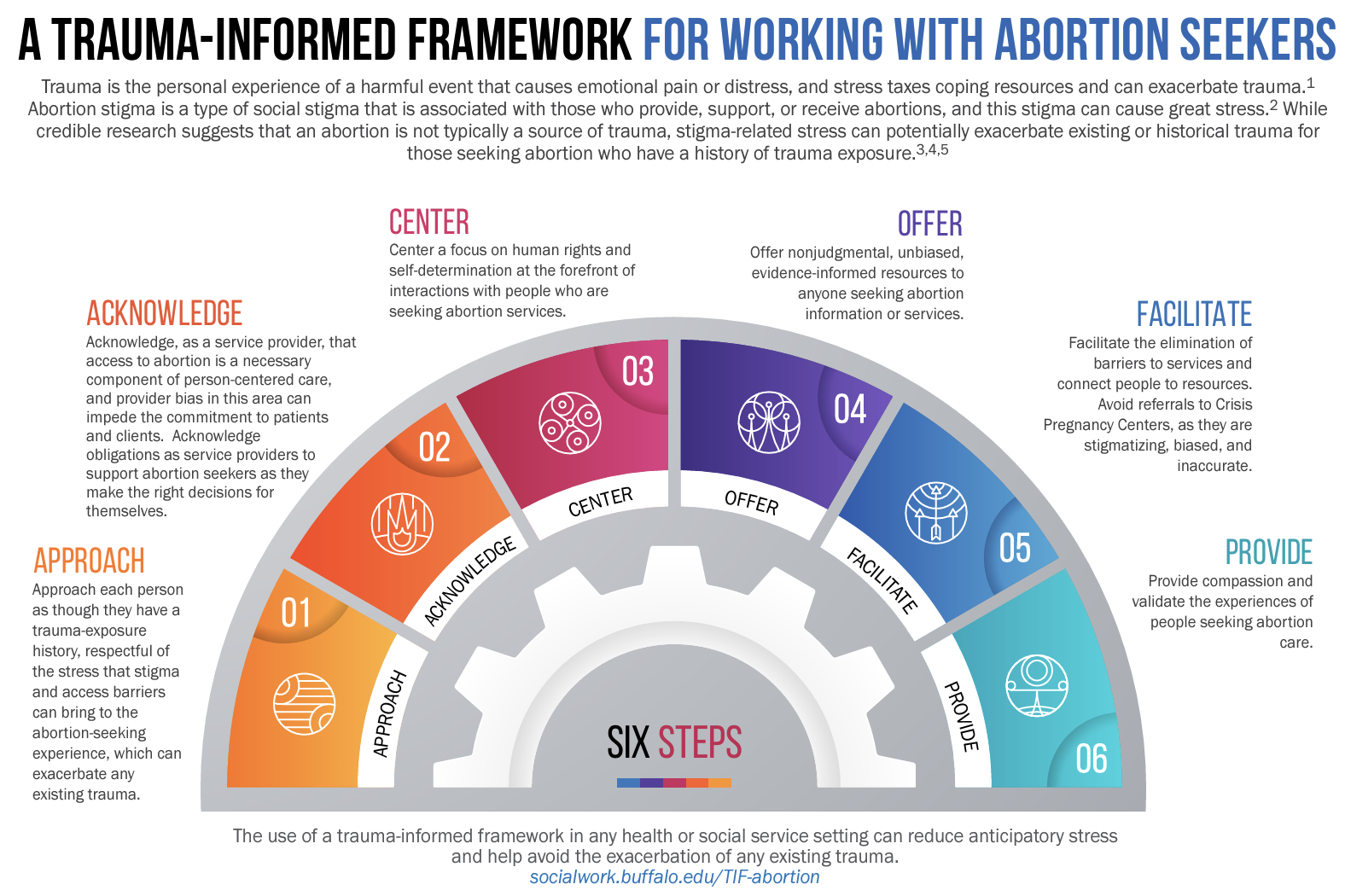
There are several tools and resources available to assist advocates in having conversations with survivors that are affirming. For example, consider using a trauma informed framework for working with abortion seekers, or Provide’s pregnancy referrals toolkit to navigate pregnancy options conversations.
“I think they should talk about it, because a lot of girls are in a situation they don’t want to be in, and abortion is not an easy subject. Having somebody just say openly, ‘Are you considering adoption? Are you considering abortion?’ will be easier on a lot of girls who are very unsure and worried about what people are going to say.” - Client feedback on the impact of abortion referral
The following organizations can provide support to people currently facing legal trouble surrounding a pregnancy or information for those who want to know how to protect themselves from being penalized by the government in pregnancy-related situations.
- If/When/How: Lawyering for Reproductive Justice: If/When/How’s mission is to transform the law and policy landscape through advocacy, support, and organizing so all people have the power to determine if, when, and how to define, create, and sustain families with dignity and to actualize sexual and reproductive wellbeing on their own terms.
- Repro Legal Helpline: A free, confidential source that has information about the law and self-managed abortion, and also connects pregnant people to lawyers if they have been investigated or arrested for having an abortion or think they may be. Visit org or call (844) 868-2812.
- FAQs on Self-Managed Abortion
- Patient Confidentiality and Self-Managed Abortion: A Guide to Protecting Your Patients and Yourself
- Real People Have Real Reasons
- Pregnancy Justice: A nonprofit organization that works to secure the human and civil rights, health, and welfare of all people, focusing particularly on pregnant and parenting women, and those who are most likely to be targeted for state control and punishment—people of color, those with low-income, and those who use drugs.
For training and technical assistance for healthcare and social service professionals and their agencies on how to destigmatize abortion and create an environment where clients feel comfortable discussing all of their options, contact Provide. They offer virtual and in-person training and capacity building support for free.
The following resources provide information to people to help them safeguard their health and understand legal risks. These organizations are well-vetted sources of information for those seeking to end an early pregnancy outside of a clinic setting, either because they lack access to legal abortion or simply want to manage their own abortions independently.
- M+A Hotline: This free, confidential, and secure phone and text hotline is staffed by doctors with years of experience caring for miscarriage and abortion. For expert advice on self-managing a miscarriage or abortion, call or text 1-833-246-2632 from 10 a.m. to 10 p.m. in all U.S. continental time zones and they will respond within an hour.
- Self-Managed Abortion; Safe and Supported (SASS): The U.S. project of Women Help Women that provides health information about self-managed abortion with pills. This support service provides information and one-on-one support for those in the U.S. looking to end their own pregnancies. SASS can connect pregnant people with experienced counselors—who are directly advised by OB-GYNs and experts on medication abortion—and can help them decide whether they’re a good candidate for self-managed abortion and other medical referrals. Email info@womenhelp.org.
- Plan C Pills: In 2017, Plan C ordered abortion pills from 14 websites without a prescription and tested the pills they received. Plan C’s website lists these results in a “report card,” which rates the reliability of the medication purchased on various websites, including information about pricing, shipping times, and amounts of active ingredients in the drugs received.
- Aid Access: Information and consultation for receiving medication abortion by mail.
- Women on Web: Founded in 2005, Women on Web is a team of medical doctors, researchers, activists, and help desk members working to provide safe, accessible, and affordable abortion care to people around the world. Consultations can be made on their website to receive pills through the mail. Email info@womenonweb.org.
- Reprocare Healthline: Provides emotional support and information for people planning or having an abortion at home. Calling is anonymous, secure, and private. Call 1-833-226-7821 from 12 p.m. to 12 a.m. PST, 7 days a week.
- Recognizing & Avoiding Unethical Facilities: “It’s important that people understand their options and know their resources—including how to recognize and avoid facilities, such as crisis pregnancy centers (CPCs), run by people who operate unethically and with the intention to dissuade, deter, or prevent them from seeking certain reproductive health care options.”
Please Keep in Mind!
By Cassandra Aho, Director of Health Equity with the National Resource Center on Domestic Violence
In alignment with our mission and values to support fully informed, autonomous decision making, NRCDV must address that the safety of SMA with Misoprostol (alone or in combination with mifepristone) does not mean that it is without risk or possible adverse reactions.
While these medications have been proven to be overwhelmingly effective treatments for SMA before 10-week gestation, it is recommended that folks consult with their provider if they are not able to accurately identify gestational age or have known conditions such as a history or risk of ectopic pregnancy, certain blood conditions such as low iron or are at risk of Rhesus Factor (Rh) incompatibility or any other health conditions that may be affected by these medications.
A few other potential risks that may require urgent medical intervention are an incomplete abortion, uterine rupture or injury, hemorrhage, infection, blood clots remaining the uterus, or allergic reaction to one or both medications.
If the pregnancy is not terminated and is carried to term, there is risk of congenital malformations of the fetus if carried to term (Planned Parenthood, n.d.; Gynecology, 2020; Verma, N., & Grossman, D., 2023).
With the ever-changing landscape of reproductive rights and abortion bans, there may also be great legal risk to a SMA depending on your geographical location.
For more information about medicinal abortions or help finding a provider in your area, please visit the websites below:
For culturally specific healthcare providers:
For legal resources or support: